A research project was recently allocated 25 million Norwegian kroner. In the project description, research results are presented on misleading graphs and presented as favorable and remarkable even though they are negative and without significance. The project hypothesis has been refuted by the researchers themselves.
This is a translation of the Norwegian text: 25 mill. til forskning – og hvordan lyve med grafikk.
There was a big uproar in 2020 when the newspaper Aftenposten had misused statistics in an article about sick leave. The graphs were truncated. If you truncate the vertical y-axis in a graph to an excessive extent, the result can be an increase or decrease that looks much steeper than reality.
A short course in how to lie with graphics, Sven Egil Omdal wrote on Facebook. The newspaper Journalisten also covered the case: “Trine Eilertsen apologizes for misuse of statistics in A-magasinet”.
The following year, a research article from a Norwegian study was published, in which participants had been treated with cognitive behavioral therapy.
Truncated graphs
The researchers had done the same thing: truncated the graphs so that the results looked much better than reality.
They conclude that cognitive behavioral therapy improves physical function and fatigue in mild to moderate chronic fatigue.
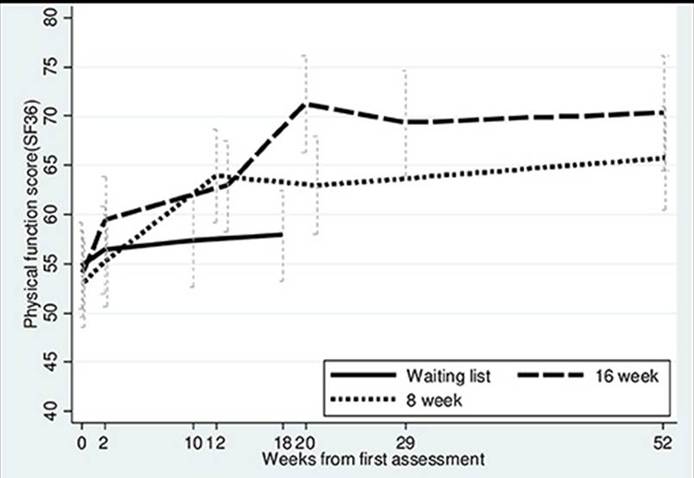
The results of changes in physical function and fatigue are illustrated with the SF-36 Physical Function Subscale graph. The scale runs from 0-100.
The graph is truncated and thus gives the impression of large changes where there are only clinically marginal effects.
Figure 2 in the article: «Primary outcome, physical function SF-36 up to 52 weeks» shows the results in a truncated Y-axis from 40 to 80:
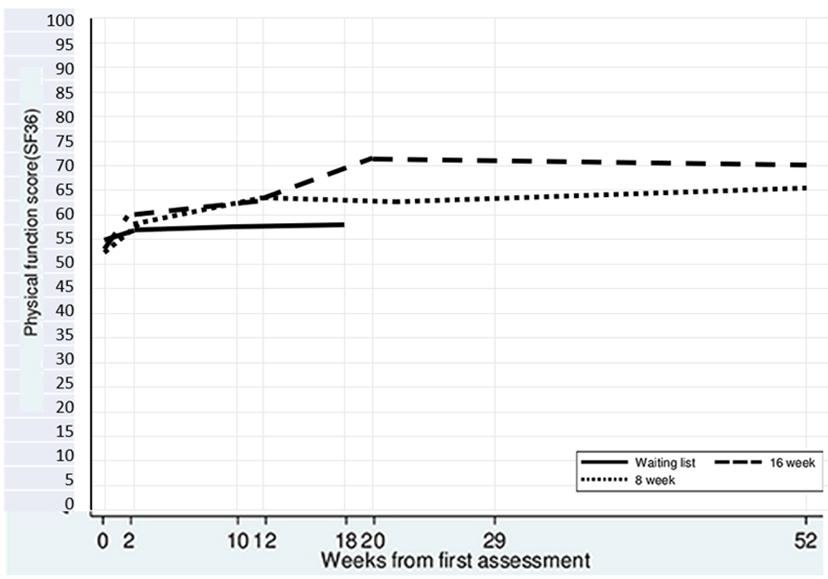
The figure below shows the same results entered into the full SF-36 scale from 0-100:
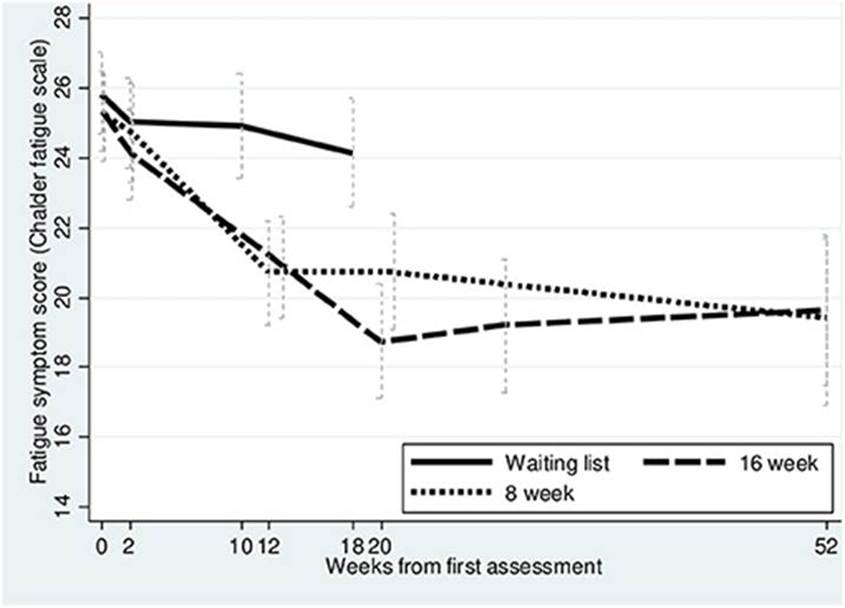
The same applies to the graph in figure 3. The Chalder Fatigue Scale runs from 1 – 33.
Figure 3 in the article “Secondary outcome, fatigue (CFQ) up to 52 weeks” shows the results in a truncated Y-axis from 14 – 28:
The figure below shows the same results entered into the entire scale from 1-33.
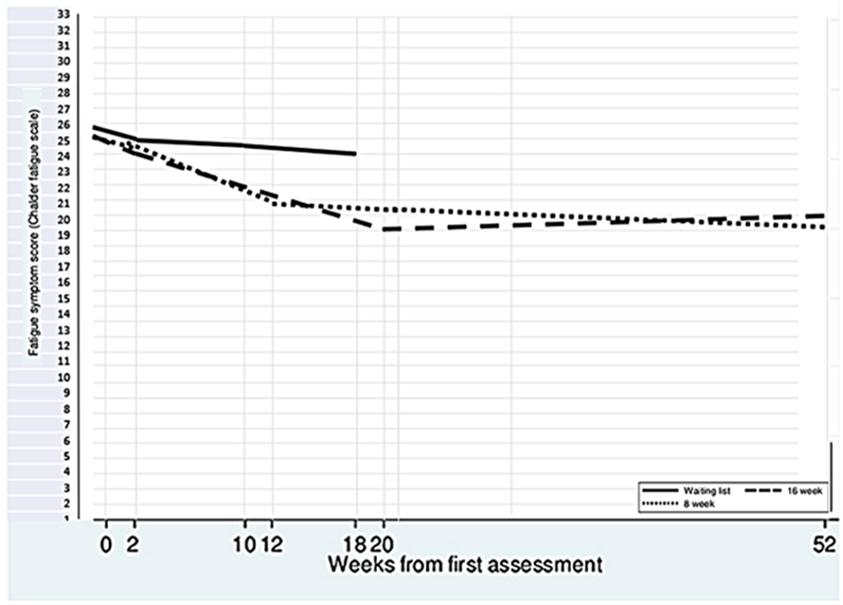
The graphs above show subjectively measured changes, i.e. personal understanding and assessment, rather than objectively measured data. The marginal changes shown by the graphs with full Y-axes could therefore just as easily reflect chance or the Hawthorne effect.
25 million Norwegian kroner
The interregional CEO meeting recently decided to allocate 25 million Norwegian kroner to the project «Rehabilitation from Persistent Fatigue (REHAB-FATIGUE): A Multi-Centre Transdiagnostic Randomized Clinical Trial». Read the project description here. The allocation was made via KLINBEFORSK; a program that announces research funds for clinical research within all disciplines in the specialist health service.
The project description claims that:
“However, the brain’s “fixed priors” are amendable through unconscious learning processes, providing an explanation for studies showing that cognitive-behavioural treatment approaches significantly attenuate symptoms and disability in postinfective fatigue conditions (such as Long COVID), 25,40 post-cancer fatigue, 13 fatigue in inflammatory bowel disease, 18 and ME/CFS.19 Data from our own research group support these findings (Fig. 3).”.
To document the claim, reference is made to the study above – with the truncated graphs; Gotaas ME, et al. Front Psychiatry 2021;12:580924.
But this is not the only one.
MINIRICO and SIPCOV
The same is done in the project description’s presentation of the results of the MINIRICO and SIPCOV studies – which are also used as an argument in the application.
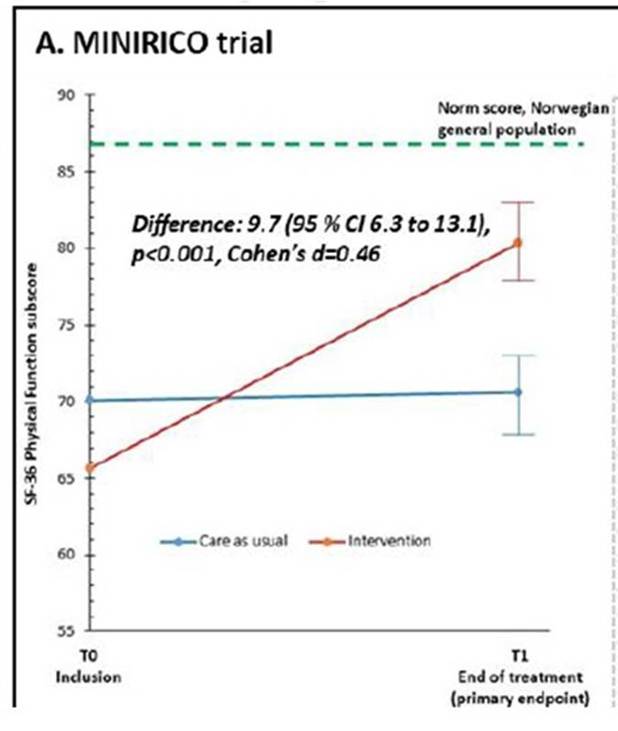
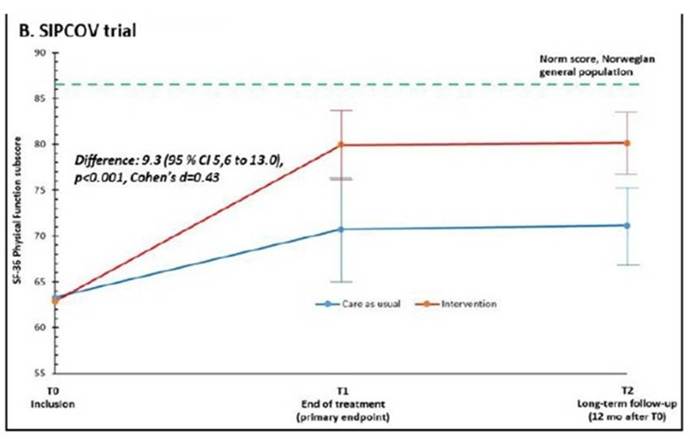
It is claimed that “A recently completed randomized clinical trial (MINIRICO) of a brief cognitive behavioral intervention (mind-body reprogramming therapy, MBRT) versus treatment as usual in long-term COVID showed a beneficial effect on physical function as well as other measures of symptoms and capacity. Similarly, another trial (SIPCOV) of a similar brief cognitive behavioral intervention in long-term COVID showed remarkably similar beneficial effects with sustained effects over time.”.
The Y-axis is truncated in both graphs to illustrate the results.
The MINIRICO study: The graph shows the result in a truncated Y-axis from 55 – 90:
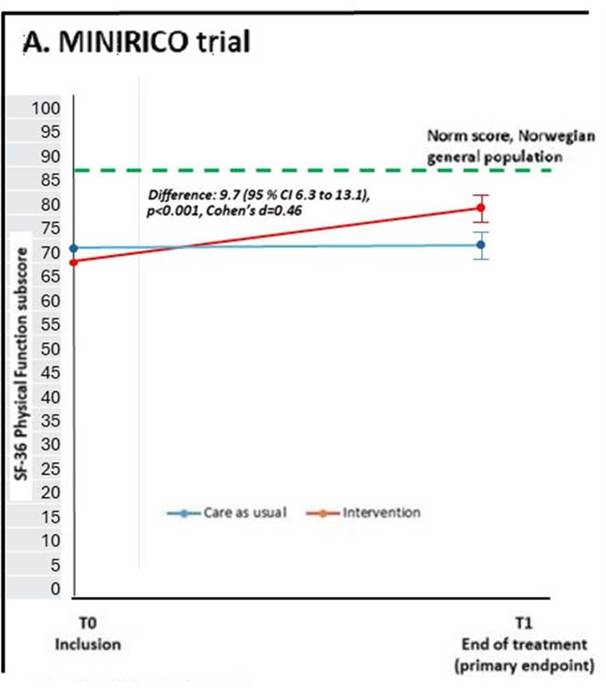
The graph below shows the same results on a full scale from 0 – 100:
SIPCOV study: The graph shows the result in a truncated Y-axis from 55 – 90:
The graph below shows the same results on a full scale from 0 – 100:
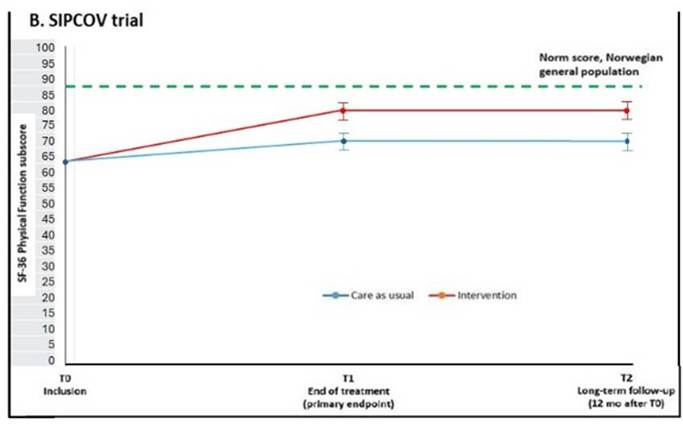
The results are thus presented as dramatically much better than reality.
Negative results in previous studies
Both MINIRICO and SIPCOV had negative results.
The Minimal Clinically Important Difference, MCID for clinically significant change for the respective SF-36 is 10 points according to the researchers themselves. Both studies received 9.x in difference between the groups. Which means that the results of the SF-36 are below the limit for clinically significant change.
The objective measurements in MINIRICO show no difference whatsoever between the groups.
This is presented in the project description as «favorable» and «remarkable» – a peculiar claim in light of the actual results. The MINIRICO study has not even been published yet.
Refuted hypothesis
The project hypothesis is that a “flawed brain network activation triggers a bodily stress response” leads to long-term fatigue. The hypothesis is in line with project leader, Professor Vegard B. B. Wyller’s sustained arousal theory from 2009 – and which was recently refuted.
Wyller et al. have studied «The relationship between hair cortisol levels, Epstein-Barr virus infections and chronic fatigue in adolescents». The report was published on March 2, 2026.
They found that higher stress levels (measured by cortisol) are not associated with the risk of developing chronic fatigue. They hypothesized that:
1) high levels of cortisol/stress before infection would increase the risk of chronic fatigue after infection, and that 2) those with chronic fatigue had lower cortisol levels than those without.
For 1) they found no association. For 2) they found similar levels between healthy controls and those with chronic fatigue.
The researchers discuss:
“Lower hair cortisol and diminished parasympathetic responsiveness may reflect a state of chronic stress, as postulated by the “sustained arousal” theory of chronic fatigue (Wyller et al., Citation2009). However, contrary to that theory, our findings suggest that symptomatic fatigue precedes these physiological changes rather than resulting directly from them. Thus, rather than sustained arousal or stress being the primary cause of fatigue (as the sustained arousal model and some biopsychosocial accounts propose), our data indicate that the development of fatigue and its associated symptoms may lead to subsequent sustained arousal/stress.”
The article does not say anything about why the samples – which were collected in 2015 – have not been analyzed and published earlier.
Read more here: Did Wyller refute his own stress theory?
A huge amount
The theoretical basis for the project that has received 25 million Norwegian kroner to study Mind-Body Reprocessing Therapy in chronic fatigue is therefore significantly weakened.
It may seem that the decision to award is based on an exaggerated and misleading presentation of research results as well as a hypothesis that the researchers themselves have refuted.
Therefore, the information above was sent to the four CEOs who approved the award, respectively Terje Rootwelt, Inger Cathrine Bryne, Marit Lind and Jan Frich.
They have asked KLINBEFORSK to respond.
Head of department Research and Diagnostics Unit at the South-Eastern Regional Health Authority Torunn Berge responds on behalf of KLINBEFORSK’s program administration:
«We are well aware of both the strengths and weaknesses of this type of application process, but it represents a well-known and proven mechanism for distributing research funds. The announcement process assumes that we use criteria that have been established in advance of the application process, and we cannot introduce new elements in the assessment during the process or after the decision.
Regarding the research articles mentioned, we would like to emphasize that these have also been peer-reviewed and published in scientific journals. This means that the methodology, analyses and conclusions have been assessed by independent experts in line with standard scientific practice. There will be different ways to present the data in question, but it is neither the administration’s nor the review committees’ task to follow up on peer reviews made by others for publication in reputable journals.
We have noted the content of your input, but it is the established review mechanism, including the peer review and the criteria that form the basis for competitive award, that are considered a sufficient basis for decision-making.».
Read the full answer here.
KLINBEFORSK is funded with an annual allocation from the State Budget via the Ministry of Health and Care Services. NOK 25 million is an enormous amount. There is negligible research funding allocated in the field in relation to the burden of disease and societal costs. Given that it is ME patients and their caretakers who finance biomedical research in the field, it is important that the research is of solid quality and based on truthful arguments.
.
Written by
Nina E. Steinkopf
Former HSEQ Chief Executive
Now; ME patient and writer

{kind=link}